|
|
Posted By Janet Hamilton,
Friday, April 24, 2015
Updated: Friday, April 24, 2015
|
Providers are sharing data more quickly with local health departments, and when disease is spreading quickly, time is important.
Electronic information sharing has been crucial to support our response to our current measles outbreak where we have identified four measles cases in two neighboring Florida counties so far. Historically, data shared from providers was mostly paper and usually took days to get into the hands of public health officials. Now the data is electronic and it is shared in almost real time. We are using our syndromic surveillance system to look for new measles cases that may not have already been reported; review our immunization registry to rapidly identify high priority contacts of the cases to target exclusions and offer disease preventing prophylactic treatment; and when suspected infections been identified, we are getting crucial confirmatory laboratory results back electronically right into our disease surveillance system within hours of results. The system is saving public health workers time and allowing us to do a better job protecting the community as we work to halt the spread of measles.
This shift (from paper to electronic information sharing) is due in large part to the American Reinvestment & Recovery Act (ARRA), which includes many measures to modernize our nation's infrastructure, one of which is the "Health Information Technology for Economic and Clinical Health (HITECH) Act.” The HITECH Act supports the concept of electronic health records - meaningful use [EHR-MU], an effort led by Centers for Medicare & Medicaid Services (CMS) and the Office of the National Coordinator for Health IT (ONC). HITECH proposes the meaningful use of interoperable electronic health records throughout the United States healthcare delivery system as a critical national goal.
While bringing about national adoption for any federal program is a difficult endeavor, implementation of new EHR reporting is gaining widespread adoption. The EHR Incentive Program incentivizes eligible hospitals and other entities for meaningfully using health IT as well as reporting electronic data on three public health measures: (1) immunizations, (2) syndromic surveillance, and (3) reportable laboratory results. The program differentiates between eligible hospitals and eligible professionals, and the listing of stage 2 public health objectives for each are below.
|
|
|
|
Eligible hospitals reporting these three measures have gained momentum over the course of 2014. New EHR Incentive Program data show that 72 percent of stage-2 hospitals reported on all three public health measures.
The ONC recently put out a data brief called Hospital Reporting on Meaningful Use Public Health Measures in 2014. The data are encouraging: |
- Almost nine in 10 stage 2 hospitals were able to electronically report to their immunization registry
- Three quarters of stage 2 hospitals reported syndromic surveillance data electronically to their local public health agency
- More than eight in 10 stage 2 hospitals submitted laboratory results electronically to their local public health agency
|
The brief goes on to project that as more hospitals shift to stage 2 in coming years, it can be expected that electronic exchange between hospitals and public health agencies will likely increase. The ONC data brief also found that when reporting was optional instead of mandatory, fewer hospitals shared public health data with local health department officials: “While almost three-quarters of stage 2 hospitals reported, without exclusion, on all applicable public health measures, only 5% of stage 1 hospitals did the same.” As hospitals and public health departments progress to interoperability, everyone will get better data in a more timely way. Sharing of data in standardized electronic formats will improve population health, help contain dangerous outbreaks more quickly and result in better patient care coordination.
Proposed MU stage 3 objectives, the third and final phase of the MU incentive program, is currently out for public comment. CSTE will be preparing comments through the Surveillance and Informatics Steering Committee. Please join us to help craft our response as well as consider submitting responses directly from your health department. |
|

Janet Hamilton, MPH serves as the Surveillance/Informatics Steering Committee Member-at-Large on the CSTE Executive Board and Surveillance and Surveillance Systems Manager at the Florida Department of Health. To learn more about surveillance and informatics, please join a subcommittee. |
| |
Are you a member with an important message to tell the CSTE community? Tell us about it!
Do you use social media? Stay tuned to CSTE on Facebook and Twitter for daily updates! |
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Emily Holubowich,
Sunday, April 19, 2015
Updated: Friday, April 17, 2015
|
| Emily Holubowich, Senior Vice President at CRD Associates is CSTE’s Washington representative and leads our advocacy efforts in the nation’s capital. Emily also serves as the Executive Director of the Coalition for Health Funding and founding Co-Chair of the NDD United campaign, both of which CSTE supports. |
|
|
|
| A rising tide lifts all boats. This familiar phrase is especially true in the current political and fiscal environment, where macro policy decisions—made behind closed doors, by a handful of powerful lawmakers, in the eleventh hour—have dramatic effects on even the most micro policy priorities. Sequestration is probably the best example of this fact—or maybe, that a receding tide grounds all boats. |
Between 2013-2021, sequestration’s harmful cuts shrink the amount of appropriated funding available for epidemiology, public health, and all core government functions by $1 trillion.
|
Between 2013-2021, sequestration’s harmful cuts shrink the amount of appropriated funding available for epidemiology, public health, and all core government functions by $1 trillion. During the last two years, we have experienced some temporary and partial sequestration relief, thanks to the Bipartisan Budget Act of 2013 negotiated by Rep. Paul Ryan and Senator Patty Murray. But sequestration returns full bore in 2016, and unless Congress acts to stop it, overall funding levels for appropriated programs, such as public health, will be 17 percent less than they were in 2010, in real terms. Under this scenario, it will be difficult if not impossible for any boats to rise. |
For information about sequestration and its effects,
click here for a primer from the Center on Budget and Policy Priorities.
|
When there’s more health funding to go around, the better the chances that our own health funding priorities—ELC grants, workforce development—do well, and vice versa (case in point: the elimination of $15 million in public health workforce funding in 2013 when sequestration first took effect). That’s why for many years CSTE has augmented our advocacy efforts to keep our own epi boat afloat by joining with our partners in the community to ensure a strong and sustained investment in health funding, writ large.
Celebrating its 45th year, the Coalition for Health Funding is the leading voice for a strong and sustained investment in the health continuum—from public health to health research and primary care services to health workforce. CSTE and 95 other national health organizations, including Association of State and Territorial Health Officials (ASTHO), National Association of County and City Health Officials (NACCHO), and Society for Healthcare Epidemiology of America (SHEA) among them, work through the Coalition to educate lawmakers about the value of health programs and the impact of funding cuts. In July 2014, CSTE contributed a story about the erosion of ELC funding for vector-borne disease surveillance to the Coalition’s report, Faces of Austerity: How Budget Cuts Hurt America’s Health. The report was shared with and has been used by lawmakers, the administration, and the media. Our story and those of other Coalition partners are available at www.cutshurt.org.
CSTE also actively participates in the Coalition’s NDD United campaign, named by The Hill newspaper as one of the “Top 10 Lobbying Victories of 2013.” NDD United is an alliance of thousands of national, state, and local organizations working across sectors to stop sequestration and protect nondefense discretionary or “NDD” programs. NDD programs are core functions the government provides for the benefit of all Americans—benefits such as public health and education, housing and social services, infrastructure and transportation, science and law enforcement, veterans services and homeland security, energy and natural resources, etc. On February 18, CSTE joined 2,100 other organizations in signing a letter coordinated by NDD United, urging Congress to stop sequestration before it returns in 2016. A copy of the letter is available here.
CSTE will continue to advocate for an end to sequestration, and for a strong and sustained investment in the nation’s disease surveillance infrastructure. For more information about these and other efforts, please contact me at eholubowich@dc-crd.com.
|
|
Are you a member with an important message to tell the CSTE community? Tell us about it!
Do you use social media? Stay tuned to CSTE on Facebook and Twitter for daily updates! |
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Lon Kightlinger,
Friday, April 10, 2015
|
Untitled Document
| South Dakota’s population will double this coming August—but the risk to public health will quadruple. The Sturgis Motorcycle Rally happens every year in the Black Hills of South Dakota attracting about 500,000 rally-goers. But this year, 2015, marks the rally’s mythical 75th anniversary and over a million Harley-stomping pilgrims are expected. Although not nearly as massive as India’s Kumbh Mela gathering, the Sturgis Rally presents vast challenges to public health surveillance and response. |
|
|
|
Sturgis (normal population 6,600) is situated where the prairie’s endless horizon meets the Black Hills, sacred to the Lakota Sioux, home to Mount Rushmore and Crazy Horse monuments, and the winding roads cyclists love. South Dakota is a rural, conservative, no-frills state that welcomes the annual boisterous mass gathering of rumbling, kick-back fun. Rally-goers come from all over the world, including far-off, exotic places like California and Pennsylvania. Catering to the million motorcyclists is an army of temporary food and drink vendors, mechanics, ad hoc camp grounds, tattooists, musicians, masseuses and more, much more. Although most rally-goers are mild-mannered gentlefolks on their home turf, while in Sturgis they let their inner Easy Rider rage for the week-long party.
The South Dakota Department of Health recognizes the risk to public health a million raucous guests might encounter: summer heat, tainted food, West Nile mosquitoes, clunker drugs, excessive Natty Ice, prairie wind storms, bothered rattlesnakes, condom scarcity, daredevil cyclist traumas, no helmet laws, 80 mph speed limits, porta-potty insufficiency, forest and prairie fire alerts, contaminated water in campgrounds that are normally cattle pastures, and old men doing things not even young cowboys should attempt.
For some this is a week of grand cycling in the Wild West, but for us in public health it is an epidemiologic OK Corral. Before and during the rally we sample, test, and enforce drinking water standards; inspect and license food venders, tattooists, and body piercing artists; implement intensive disease surveillance; activate a mobile laboratory; maintain redundant communication channels; participate in the rally emergency operations center; monitor disease cases, syndromes, hospital beds, emergency department traffic, blood supply, and morgue space; and spray for mosquitoes. The capacity of the Department of Health is stretched and local health care is overextended, as are roads and normal infrastructure.
Surveillance and response networks have been long established and work well, but the glut of accidents, cases and sudden health events engulfs and strains the disease reporters and coders in the healthcare system so that even electronic syndromic surveillance triggers are less reliable. Disaster epidemiology tools used during floods, blizzards and tornadoes need to be enhanced and envisioned for a highly mobile, raucous, wittingly uncooperative crowd who would simply not allow an outbreak of diarrheal disease to disrupt the revelry. |
|

Lon Kightlinger, MSPH, PhD is state epidemiologist at the South Dakota Department of Health. |
|
| Learn more about the various epidemiologic domains impacted by massive events, such as the Sturgis Rally, by joining a subcommittee in Surveillance and Informatics, Occupational Health, Injury, and Infectious Disease. |
|
Are you a member with an important message to tell the CSTE community? Tell us about it!
Do you use social media? Stay tuned to CSTE on Facebook and Twitter for daily updates! |
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Alfred DeMaria, Jr.,
Tuesday, April 7, 2015
Updated: Thursday, April 2, 2015
|
|
 For the 2015 Annual Conference, CSTE is pleased to announce Dr. Paul Farmer as the Jonathan Mann Memorial Lecturer. Dr. Farmer obtained an M.D. and Ph.D. in anthropology from Harvard University, and is board certified in internal medicine and infectious diseases. He is the co-founder of an international social justice and health organization, Director of Partners in Health, and is renowned for his years of nonprofit leadership, numerous awards, and insightful publications on global health. Read Dr. Farmer’s biography on the conference website. For the 2015 Annual Conference, CSTE is pleased to announce Dr. Paul Farmer as the Jonathan Mann Memorial Lecturer. Dr. Farmer obtained an M.D. and Ph.D. in anthropology from Harvard University, and is board certified in internal medicine and infectious diseases. He is the co-founder of an international social justice and health organization, Director of Partners in Health, and is renowned for his years of nonprofit leadership, numerous awards, and insightful publications on global health. Read Dr. Farmer’s biography on the conference website.
|
| We are also pleased to announce the following plenary speakers: |
- Mary T. Bassett, MD, MPH: Commissioner of the New York City Department of Health and Mental Hygiene
- Devra Lee Davis, PhD, MPH: Founding Director of the world’s first Center for Environmental Oncology and President of the Environmental Trust
- Richard Jackson, MD, MPH: Professor of Environmental Health Sciences at University of California, Los Angeles and former Director of the CDC National Center for Environmental Health
- Anne Schuchat, MD: Director of the CDC National Center for Immunization and Respiratory Diseases and Assistant Surgeon General of the United States Public Health Service
- Nancy Krieger, PhD: Professor of Social Epidemiology at Harvard University
- Pardis Sabeti, MD, DPhil: Associate Professor at the Center for Systems Biology at Harvard University
|
|
|
|
| The 2015 Annual Conference in Boston will span four days with 240 sessions on emerging topics. Some of this year’s topics include: |
- Advanced molecular detection to improve food safety
- Respiratory diseases, Chikungunya, measles, shigellosis Enterovirus D68, and Ebola
- Health impacts for 9/11 rescue and recovery workers
- Maximizing the benefits of advances in informatics
- Marijuana-associated hospitalization rates and usage surveys
- Novel approaches to collecting data with hard-to-reach populations
- Addressing the challenges of Hepatitis C surveillance
- Climate change and environmental impacts on disease
- Addressing quality of life in older adulthood
|
|
In addition to the wide array of rapid-fire, breakout, and plenary sessions, you’ll have the opportunity to participate in a variety of activities. Conference festivities include the opening reception, connections reception, and 5K walk/run. There is also a banquet at additional cost. CSTE will present awards for outstanding leaders, partners, fellows, mentors, poster presentations, and more.
This year’s conference features a new phone app to help you schedule sessions, connect to other attendees, see conference news alerts, access an interactive floorplan, and learn local information for restaurants and activities around the Hynes Convention Center.
If you register for the conference before May 1, you can receive the early-bird discount. If you aren’t already a member, joining CSTE will allow you to get the most out of the conference experience, develop your professional capacity, network, and more. The many benefits of yearlong membership are highlighted in this new video:
|
|
https://www.facebook.com/video.php?v=1040282089318703 (Please watch in HD)
|
|

CSTE President Alfred DeMaria, Jr., MD is state epidemiologist of Massachusetts. For more information about the 2015 CSTE Annual Conference, please visit http://www.csteconference.org.
|
| |
|
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Jeff Engel and Chad McCoull,
Friday, March 27, 2015
Updated: Friday, March 27, 2015
|
Untitled Document
CSTE meetings show progress for federal program partnerships and promise for Congressional appropriations.
This week CSTE leadership met in our nation’s capital to make recommendations based on the needs and perspectives of state and local epidemiologists. Executive Board members Al DeMaria of Massachusetts, Tim Jones of Tennessee, and Janet Hamilton of Florida were accompanied by CSTE Executive Director Jeff Engel, Washington Representative Emily Holubowich, and Communications Coordinator Chad McCoull. |
|
|
|
| Meeting with our colleagues in the executive and legislative branches provided a forum to share data and stories about both the challenging day-to-day realities and heartening accomplishments of applied epidemiology in America. These continued discussions help align federal priorities with those of state and local health departments in order to better alleviate burdens and bridge capacity gaps. CSTE leaders touched upon multiple recurrent topics: |
- Recommendations on national action in antibiotic resistance
- Gaps in healthcare-associated infection data collection and dedicated staffing
- Strategies for harmonizing and developing national reporting systems
- Assessment results in workforce capacity and fellowship programs
- Institutional perspectives on Ebola Virus Disease monitoring programs
- New directions for the Emerging Infections Programs (EIP) network
|
| In addition to these illuminating discussions, CSTE presented a joint letter, coproduced with the Association of Public Health Laboratories and addressed to legislative subcommittees that preside over public health appropriations. The letter urges continued bipartisan support for core epidemiology activities, emerging priority areas, and more: |
- Emerging and Zoonotic Infectious Diseases
- Combating Antibiotic Resistant Bacteria (CARB)
- Epidemiology and Laboratory Capacity (ELC) grants
- Foodborne Disease Surveillance
- Advanced Molecular Detection
- Workforce and Career Development, including CDC/CSTE Applied Epidemiology Fellowships
|
|
| |
| As a direct result of this week’s meetings, CSTE is forging new partnerships to better serve its national membership. CSTE looks forward to further opportunities to work with the Office of Management and Budget and the Office of the National Coordinator for Health Information Technology (ONC) as well as the Centers for Disease Control and Prevention Washington, D.C. office and CDC National Center for Health Statistics. As public health practitioners at all levels of government come together to shape the future of epidemiology, CSTE remains a unifying voice for the national public health applied epidemiology workforce. |
| |
| Jeffrey Engel, MD is Executive Director and Chad McCoull, MPA is Communications Coordinator at CSTE. CSTE members with messages they wish to share with CSTE leaders are welcome to contact us. For more information on CSTE’s advocacy efforts, read Emily Holubowich’s CSTE Features article on President Obama’s proposed fiscal year 2016 budget. |
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Andrew Beron, Whitney Clegg, and Justin Albertson,
Friday, March 20, 2015
Updated: Friday, March 20, 2015
|
Untitled Document
 Measles is a highly contagious vaccine-preventable disease that typically presents with a high fever and characteristic rash. Although it was declared eliminated from the United States in 2000, measles outbreaks still occur among unvaccinated children and adults due to importation of cases from countries where the disease remains endemic. As CDC/CSTE Applied Epidemiology fellows at the Illinois Department of Public Health, along with former CSTE fellowship alum Kelley Bemis, we had the unusual opportunity to respond to a measles outbreak connected to a suburban Chicago childcare center. Measles is a highly contagious vaccine-preventable disease that typically presents with a high fever and characteristic rash. Although it was declared eliminated from the United States in 2000, measles outbreaks still occur among unvaccinated children and adults due to importation of cases from countries where the disease remains endemic. As CDC/CSTE Applied Epidemiology fellows at the Illinois Department of Public Health, along with former CSTE fellowship alum Kelley Bemis, we had the unusual opportunity to respond to a measles outbreak connected to a suburban Chicago childcare center.
In January 2015, Illinois public health officials were notified of an adult with a febrile rash who tested positive for measles. This individual reported an unknown vaccination history and denied recent travel or exposure to ill individuals. By the middle of February, 14 additional measles cases had been identified. Twelve of these cases were infants that attended the same childcare center and were not old enough to receive the measles, mumps, and rubella (MMR) vaccine. Although no definite link to the index case was established, all cases resided in the same geographic area or attended childcare there. Of the 14 cases that were laboratory-confirmed PCR positive by the Illinois State Public Health Laboratory, nine were genotyped and found to be measles genotype B3. This genotype was also identified in a recent multistate outbreak linked to a Disney theme park in California and a large outbreak in the Philippines. The genotype has been detected in at least 14 countries and six U.S. states in recent months..
After the first case was identified, a public health investigation was initiated to prevent further spread of the virus in the affected communities. Because measles is highly infectious, it was necessary to perform extensive contact tracing and obtain thorough travel histories for each infected individual. We worked to determine locations each of the individuals visited during their infectious period. Identified exposure settings included places of employment, pediatric clinics, grocery stores, and other public settings.
Each location was notified about the potential measles exposure, and lists of potentially exposed individuals were compiled. For public locations, such as grocery stores, where it was difficult to identify exposed individuals, press releases were issued to notify the public. All identified contacts were asked about their vaccination status and educated about the signs and symptoms of measles. The incubation period of measles is seven to 21 days, so susceptible individuals were monitored via phone or email for three weeks following their last measles exposure.
Another critical component of the investigation involved determining the vaccination history of individuals that work with a susceptible population(s), which included employees at the implicated childcare center and healthcare workers at the exposed pediatric clinics and community hospital. We found that not all employees knew their MMR vaccination status. Not only did this lead to difficulties for the investigators, but determining employee vaccination history was a large task for the staff of the childcare center, community hospital, and affected pediatric clinics. |
|
|
|
As a result of our investigation, we were able to coordinate and implement appropriate control measures to prevent further spread of the disease. This included isolating cases during their infectious period, excluding susceptible contacts from high-risk settings, coordinating community vaccination clinics, and providing post-exposure prophylaxis to contacts when applicable.
A majority of the cases in this outbreak were among a vulnerable population. Infants are not recommended to be vaccinated with their first dose of MMR until they are 12 to 15 months of age, leaving them susceptible to measles. Young children are also at a higher risk of developing measles-related complications, such as pneumonia or encephalitis. For these reasons, vaccination of children and adults with the MMR vaccine following the recommended schedule is pivotal for protecting vulnerable individuals. Additionally, this outbreak highlights the need for those who have regular contact with vulnerable populations, such as healthcare workers and staff of childcare centers, to be properly vaccinated with documentation readily available to their employers. With the guidance and support from our mentors and colleagues, the work we accomplished in this outbreak has given us a unique and invaluable experience in the field of applied epidemiology. |
|
|
|
| Andrew Beron, MPH, Whitney Clegg, MD, MPH, and Justin Albertson, MS, are CDC/CSTE Applied Epidemiology fellows at the Illinois Department of Public Health. Visit the CSTE website to learn more about information about the CDC/CSTE Applied Epidemiology Fellowship. For more information on measles, mumps, and rubella, learn about the CSTE Vaccine Preventable Diseases Subcommittee. |
|
Are you a member with an important message to tell the CSTE community? Tell us about it!
Do you use social media? Stay tuned to CSTE on Facebook and Twitter for daily updates! |
| |
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By James Davis (NM), Jennifer Sabel (WA), Dagan Wright (OR), and Svetla Slavova (KY),
Friday, March 13, 2015
Updated: Friday, March 13, 2015
|
Did you know that drug overdoses are the leading cause of injury death in the nation? While we know that they are a leading cause of injury death, the ICD codes often only tell us the broad class of drugs involved and not the specific drugs. However, there is often more information about the specific drugs on the death certificate.
A new analytic tool developed by the CSTE Overdose Subcommittee treads new ground by directly analyzing the cause of death information on the death certificate, sometimes referred to as the literal text. Literal text entries from the death certificates are now either entered into electronic death certificates or transcribed paper certificate. These entries are used to classify the causes of death using the ICD-10. The literal text entries are input into the SuperMICAR program of the suite of software used to code the causes of death and thus these literal text entries are sometimes referred to as the SuperMICAR literal text. |
|
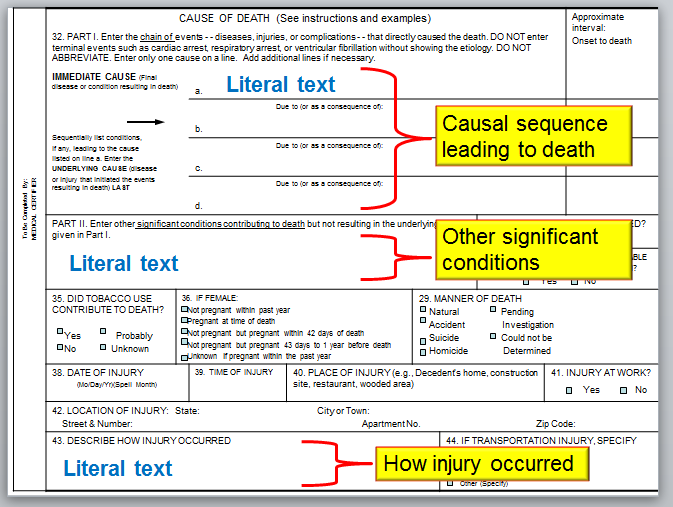 The cause of death section from the US standard death certificate
The cause of death section from the US standard death certificate |
|
This new program searches the electronic version of the literal text for references to specific drugs and other words of interest that are included in the cause of death statement and the “how the injury occurred” text box. The program creates additional variables in the data set to record the drug names and number of drugs.
After processing the literal text data with this program (and after a thorough manual review of the output), state and local analysts can learn more about the leading drugs involved in deaths in their jurisdictions. For example, the leading drugs involved may be oxycodone, methadone, heroin, and alprazolam. These data could be used for surveillance to monitor the number of deaths from a particular drug. Analysts could also use the search terms spreadsheet to monitor the literal text for new drug threats.
There are some limitations to the current program. Importantly, in some states these literal text data are restricted and may not be available to all analysts. The drug list is a work in progress and can be improved. Also, the program searches for mentions of a drug without considering the context. There are likely to be false positives; that is, a drug is mentioned, but did not contribute to the death. For instance, “insulin” is on the drug name list and would identify “non-insulin dependent diabetes.” Another example would be “heroin user” which does not necessarily imply that heroin was involved in the death. |
|
| The tool is available here on the CSTE website. We are requesting feedback though updates will be made as times permits. Please send feedback to Nidal Kram. We hope that you will take the tool and expand on it and use it in your work reviewing other causes of death. |
|
|
|
| James Davis, MA is Substance Abuse Epidemiologist at the New Mexico Department of Health. This project was prepared by the CSTE overdose workgroup on literal text analysis, including Jennifer Sabel, Jim Davis, Dagan Wright, Svetla Slavova from CSTE; Margaret Warner, Ari Minino, from NCHS; and Len Paulozzi, and Rose Rudd from NCIPC. For more information, read about the CSTE overdose subcommittee and the CSTE Substance Abuse Subcommittee. |
| |
| |








